White Paper
Optimizing Drug Life Cycle Market Performance
Summary
Most drugs do not achieve their projected revenue forecasts. While revenue strategies for pharmacy dispensed drugs are well socialized, clinically administered drugs face unique, largely unaddressed challenges associated with the nuances of medical claims processing. In this white paper, we present best practices to address the industry-wide challenges and a seven-point checklist to guide effective comparisons of alternative healthcare data analytics solutions.
By:ĚýTim SutherĚýSenior Vice President, Data SolutionsĚýµçłµÎŢÂë
Mark Cross Senior Director Strategy, Data Solutions µçłµÎŢÂë
Nicole Hobbs Market Research Analyst 5, Data Solutions µçłµÎŢÂë
Sam Woodard Product Lead Data Solutions – Life Science µçłµÎŢÂë
Introduction
Most drugs do not achieve their projected revenue forecasts. While revenue strategies for pharmacy dispensed drugs (those covered under pharmacy benefits) are well socialized, clinically administered drugs (those covered under medical benefits) face unique, largely unaddressed challenges associated with the nuances of medical claims processing.
Finding, analyzing, and acting on critical knowledge, from prelaunch to post-market, improves performance. A healthcare data analytics platform that provides this requires three assets: deidentified medical claims/remittances/SDoH data, a user-friendly drug commercialization intelligence platform, and built-in systemic compliance monitoring.
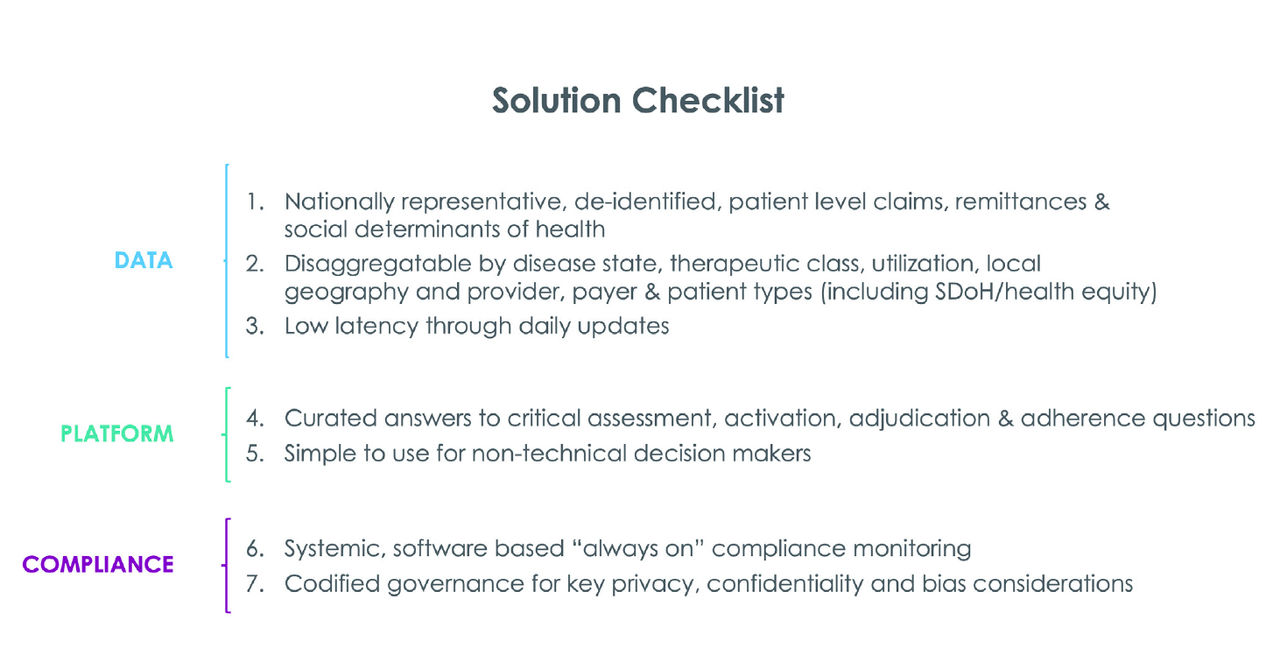
In this white paper, we present best practices to address the industry-wide challenges and a seven-point checklist to guide effective comparisons of alternative solutions.
Assessment
First year performance often establishes a drug’s long term trajectory1. Approximately 70% of products that miss launch projections continue to underperform over time. Forecasts, first year and beyond, can be informed by understanding peer drug prescribing patterns, utilization, reimbursement, denial rates, adherence, and market trajectory. While brand managers have long sought these insights, unfortunately, the underlying data foundation has been suboptimal.
Notably, for drugs planned for medical benefit coverage, assessment is notoriously complicated. A new drug can be negatively impacted by close to 2,000 denial codes, resulting from countless payer, provider, or patient decisions, each uniquely motivated. The problem continues to escalate as denial rates for the first half of 2022 accelerated 20% year over year.
While many denials are avoidable or recoverable, deciphering causes and countermeasures requires more granular data than is commonly available. It’s key to have geographically representative patient level data for both medical claims and remittances (where denials are found) to build robust billing guides for complex and expensive drugs2.
But medical claims and remittances won’t be enough: individual patient-level SDoH are also needed to understand motivations, behaviors and friction points more fully across target populations. In particular, individualized SDoH can reveal access and adherence variations across key target populations, over time, for key subsegments. Planning for these variations, as opposed to merely reacting to them, will help optimize performance.
Together, national patient-level medical claims/ remittances/SDoH provide an improved foundation to better answer important questions. How did similar drugs perform? What were the highest and lowest performing subsegments and why? What were the major friction points (access, cost, missing information, etc.) and how were they resolved? An improved healthcare data analytics foundation fills critical information gaps needed to develop clear and accurate billing guides, effective operational workflows, and training for claims submission and Electronic Remittance Advice (ERAs) interpretation.
Activation
A successful launch needs an activation plan with near-real-time stakeholder monitoring and enhanced compliance controls. Once again, drugs covered under the medical benefit require special attention. In contrast to pharmacy claims, medical claims are not adjudicated in real-time, are often intermixed with complex care, and entail substantially higher cost, all of which affect whether a new drug is approved and prescribed.
A new drug can be negatively impacted by close to 2,000 denial codes, resulting from countless payer, provider, or patient decisions, each uniquely motivated. The problem continues to escalate as denial rates for the first half of 2022 accelerated 20% year over year.
Effective activation requires access to current, detailed prescribing/reimbursement behavior. The key is to quickly assess how providers, patients, and payers, each with different circumstances, are responding to activation initiatives, ideally with enough depth to precisely detect underlying drivers.
While assessment aggregates data to forecast and invest, activation disaggregates data to detect and remediate friction in individual decision making. This can inadvertently increase re-identification risk. As it is, re-identification risk already can be under-appreciated as “expert determinations” are performed infrequently, risking non-compliance with fast-moving data and analytic needs. It’s best to replace manual determinations with systematic and automated compliance monitoring.
Adjudication
Once activated, attention turns to optimizing prescriber and patient experiences. A common abrasion point for both are claim denials. Left unattended, a denial is not only inefficient (most denials are avoidable and/or correctable) but creates risk that patients or providers decide your drug isn’t worth the trouble. And with over 1,800 medical claim denial reason codes, it can be maddening to zero in on the best strategies to minimize them.
.Benefit submission is significantly harder for clinically administered drugs. As an example, many drugs under medical benefit take weeks (or months) to adjudicate, and average 2.7 submissions before approval (some as many as 7-9 tries). Denial recovery is also expensive for providers and can cost as much as $118 to $124 to resubmit and correct3.
If left unaddressed, such friction can lead providers and patients to choose other, seemingly more convenient medication options, causing market share to decline.
Successful adjudication planning requires depth of data and low latency. Denial codes at the item level are needed, as a claim can be denied for hundreds of reasons. Latency is also important. On average, claims for the ten most popular cancer medications are open for a staggering 29 days, with one drug being open for 66 days. The earlier issues are identified, the sooner they will be resolved.
While assessment aggregates data to forecast and invest, activation disaggregates data to detect and remediate friction in individual decision making, such as claim denials and adjudication time. If left unaddressed, such friction can lead providers and patients to choose other, seemingly more convenient medication options, causing market share to decline.
Adherence
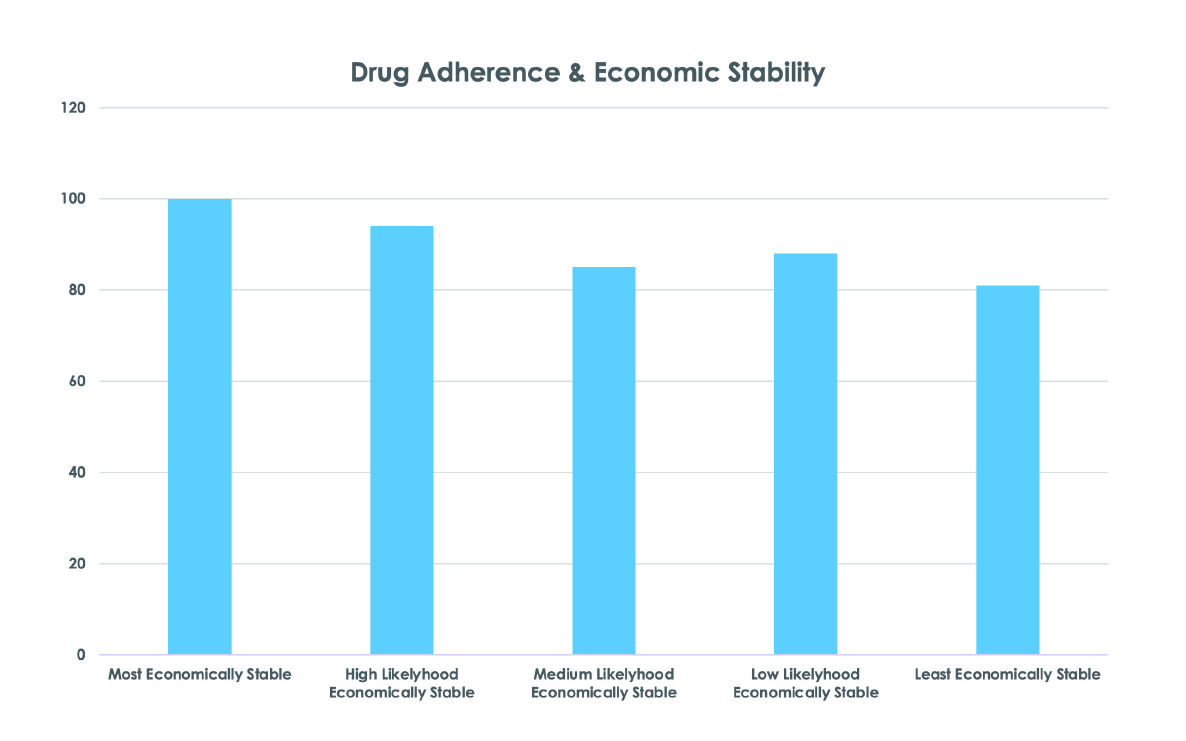
The last of the 4 A’s is adherence and remains among healthcare’s most challenging problems. Of course, the most serious impacts are experienced by patients, but non-adherence also costs pharmaceutical makers $637B globally ($250B in the United States) every year4.
Life outside of the doctor’s office greatly influences how or if patients adhere to their medications. Nonadherence is highly correlated to SDoH risks and challenges5 and leads to higher healthcare costs and worse outcomes4. Financial stability is directly correlated to adherence (see chart)X2.
Unfortunately, most adherence initiatives are limited by poor patient data. One typical approach relies upon census tract averages, which are useful for planning, but inadequate for patient support. The average economic, housing, or food vulnerability in an area tells us nothing about an individual, and often are out of date. Patient-reported data is another usual source; however, fill rates typically are low due to lack of patient incentive to share their data. Even when provided, non-standardized data can make analysis difficult or erroneous. Lastly, particular care must be taken to ensure that the patient answers truthfully.
An effective alternative is individual level, standardized, and independently verified data about the patient, as outlined in our Multidimensional Patient Journey white paper. Until standardized, self-reported data can be accurately captured, these independent datasets offer the most actionable alternative.
Capturing data about patient adherence drivers can also inadvertently increase the risk of reidentification. As noted previously, it’s best to replace manual determinations with systematic and automated compliance monitoring.
The Solution
Launching therapeutically administered drugs covered under medical benefits is fraught with difficulties. To overcome these innate issues, market and stakeholder intelligence throughout a drug's life cycle are essential. Finding, analyzing, and acting on critical knowledge, from pre-launch to post-market, improves performance. Superior execution requires three assets: de-identified medical claims/remittances/SDoH data, a userfriendly drug commercialization intelligence platform, and built-in systemic compliance monitoring.
Data
High performance starts with reliable facts. For drugs covered under medical benefit, it’s best to use national level disaggregated patient level claims and remittances appended with individualized SDoH. This data should include comprehensive rejections and denial reason codes; fill rate by pharmacy type; percentage of paid, pending and denied claims; claims reversal by pharmacy type; average days to claims resolution; and claims paid by insurer type. This level of disaggregation is necessary to fully dissect conditions causing denials.
Patient level SDoH enables better understanding of nonadherence and should include economic security, race, ethnicity, and health literacy/education. Neither census track or patient reported SDoH can provide sufficient accuracy to address access and adherence challenges. Finally, a daily data refresh is essential to respond quickly to shifting market conditions.
Platform
Facts alone are not enough: data needs to be transformed into insights that are easily accessible and usable by business decision makers. Traditionally, brand managers relied on intermediaries to manually extract and evaluate insights. Now, curated insights and usability are the key design principles of a modern drug commercialization intelligence platform, offering a more cost effective, simpler, and faster path.
Automatically curating insights across the 4 A’s are critical. Assessment intelligence decodes provider, patient, and payer behavior to better plan for, not just react to, constituent outreach, education and support. Activation intelligence enables hyperlocalized insight into how new prescription writers should be prioritized, activated, and cultivated.
Adjudication intelligence triangulates reason codes by service line relationships, payer protocols and patient journey status to detect underlying drivers. Adherence intelligence analyzes drug utilization by dose and duration across target patient populations in order to fully comprehend prescribing patterns, patient needs, and therapy efficacy by derived subsegment. A healthcare data analytics platform provides curated insights into how providers, patients and payers are responding at each of the 4 A’s.
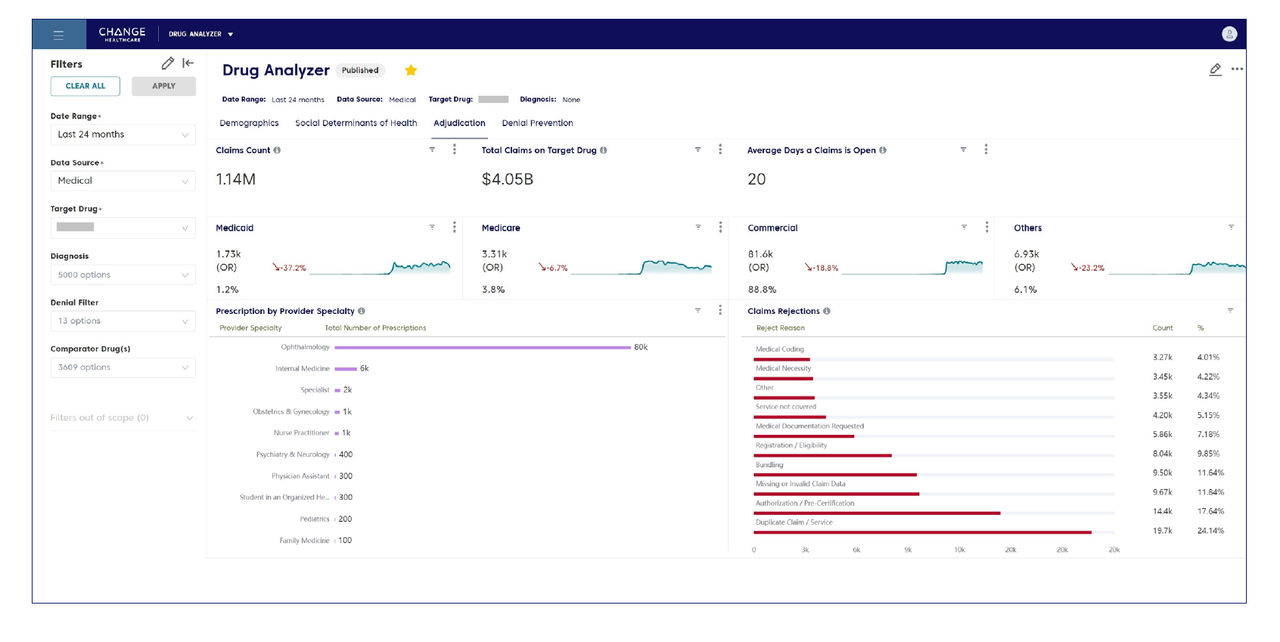
Accessibility and ease of use for business decision makers is also important. A responsive dashboard with dynamic visualization (See example below) enables a business user to intuitively find, categorize and benchmark analog drugs by disease or molecule type. It should help estimate market potential, interpret financial performance, decipher intricate prescription coding, surface major friction points, and help prioritize outreach. Bottom line, it should come pre-populated with easily accessible answers to questions affecting the rate and scale of drug performance, as asked by brand managers.
Compliance
Utilizing reliable facts and decision intelligence necessitates a third tool: systemic compliance monitoring, particularly for privacy (maintaining security and confidentiality of patient information). Compliance with HIPAA’s Privacy Rule has never been more challenging, given the accelerating diversity of available patient data (mathematically, more patient attributes increase reidentification risk6). Emerging state privacy regulations further complicate matters with inconsistent deidentification standards.
Detecting and remediating bias (disadvantaging a specific demographic group) is another important requirement in today’s health equity conscious environment. Analyses that test for representativeness in access or outcomes is foundational, and having that ability built into the platform is valuable. Leaders will possess the ability to disaggregate access and outcomes by protected class or other key population subsegments. Such granular insights are vital as part of your health equity strategy.
Because addressing compliance episodically or manually generates unnecessary risk, it is critical to implement a configurable "always on" softwarebased surveillance that monitors for privacy, confidentiality, bias and other business requirements.
Conclusion
Brand managers, under pressure to deliver quick success, are no longer constrained by third parties, manual processes, long cycle times and inadequate data. It is now possible to remove the blinders that complicate clinically administered drug launches. Healthcare data analytics solutions exist to help avoid inclusion in the 70% club, drugs that do not meet expectations. A modern drug commercialization intelligence platform with built-in compliance guardrails and the right data will provide easy access to the insights needed to overcome the physician activation, reimbursement, patient engagement, and adherence challenges inherent in medically reimbursed therapies. Our seven-point solution checklist shows the way to effectively compare alternatives.
1 Key factors to improve drug launches. Deloitte Insights .
2 Unpublished Research, µçłµÎŢÂë. (2022).
3 Measuring the Cost of Denials and the Impact of Prevention. .
4 Bulik, B. S. Nonadherence costs pharma $600B-plus in annual sales: study. Fierce Pharma
5 Wilder, M. E. et al. The Impact of Social Determinants of Health on Medication Adherence: a Systematic Review and Meta-analysis. J. Gen. Intern. Med. 36, 1359–1370 (2021).
6 Combining Large Data Sets Challenges IRBs, Researchers to Ensure…. Relias Media | Online Continuing Medical Education | Relias Media - Continuing Medical Education Publishing

